Cannedy had grown up in California and joined the Marines in 1981, at the age of 21. He didn’t see combat, but his body took plenty of punishment in service to the Corps anyway. He pole-vaulted for the track team, played football despite his slender build, boxed in Golden Gloves tournaments. He went to the emergency room with suspected concussions five times in four years. Each time he was soon back in the fray, exhibiting the seemingly endless resilience of youth.
After his discharge, Cannedy worked as a personal trainer and poured concrete. He started his own pest-control company. But after a decade or so of civilian life, he began to get confused and disorganized. He couldn’t keep track of his work schedule or who’d been billed for what. He lost his business, his house, his marriage, his family.
“I started to get into some bad places,” Cannedy says. “I ended up living in a storage shed for ten years. I’d get up and go to the gym and then drive around aimlessly. Most people didn’t realize I was homeless.”
Eventually, Cannedy was diagnosed with a traumatic brain injury. The Veterans Administration found that the TBI was service-related and granted him a 100 percent disability rating. The VA offered him rehab services, cognitive therapy and drugs, but none of it did much to help his rapidly deteriorating short-term memory. He was losing basic skills and showing early signs of dementia.
Two years ago, Cannedy moved to Austin, Texas. He took a run at some alternative approaches to TBI treatment, including hyperbaric oxygen chambers and equine therapy. The horses, like the extra oxygen, boosted his mood but had no lasting effects. Then his caregiver heard about two doctors in Colorado who claimed to have achieved encouraging results treating TBI patients with something called transcranial near-infrared laser phototherapy — a fancy term for shining a laser on patients’ noggins in the expectation that this specific form of light will trigger healing processes in the brain.
That’s how Cannedy ended up in a treatment chair at the Neuro-Laser Foundation, located in an anonymous office complex in Centennial. Over a period of weeks, he went for eleven sessions, each one lasting about forty minutes. At first he found the experience so relaxing, the gentle warmth of the light moving across his temple almost putting him to sleep, that he wondered if it was doing any good. But after a few sessions his caregiver, Michelle Beste, could see some promising signs; the thief wasn’t gone, by any means, but it was as if his progress had been slowed considerably."People are getting better. But for me, as a scientist, that's unsatisfactory. I want to be able to say why people are getting better."
tweet this
“It’s the first thing I have found that has made for some cognitive improvement,” Beste reports. She ticks off a series of simple tasks that Cannedy couldn’t manage or struggled with before the treatments and now performs with ease: He can do his laundry by himself and fold it. He can spell his name, recite his phone number, sign his name in cursive. His short-term memory seems to be improving, and he no longer thrashes about in his sleep with nightmares.
“Right now he would be in a nursing home if it wasn’t for people coming over to assist him at home,” she notes. “Any little gain he can have gives him a little more independence.”
Cannedy says the results to date have made him “incredibly happy” — and have him looking forward to more sessions. “I can live with this,” he declares. “I have such a fantastic outlook now. We’re not going to give up.”
Others who’ve made pilgrimages to Centennial to submit to the healing light tend to echo Cannedy’s optimism. The improvements they’re experiencing may seem modest to outsiders, but they’re better than no change at all. Most of all, they say, the treatments have given them something that is often in short supply among those battling severe brain injuries: hope.

Theodore Henderson (left) and Larry Morries check settings on the near-infrared laser they use to treat patients with traumatic brain injuries.
Jim Darling
Among mainstream medical researchers, such assertions have been met with a stony silence — and an occasional snort of skepticism. Some have raised questions about the size of the study group involved or whether the brain imaging technology used to document the results is less revealing than it appears to be. Henderson and Morries shrug off such carping, saying they’re in the process of raising a million dollars to fund a large-scale study that will back up their claims.
“What we’re doing looks great,” Henderson says. “People are getting better. But for me, as a scientist, that’s unsatisfactory. I want to be able to say why people are getting better. And I think that’s what we’re doing.”
Given the stakes involved, it’s surprising that the claims of a breakthrough by two maverick Colorado researchers have garnered so little attention. Traumatic brain injury is a growing problem not only for athletes, but for the population at large, with an estimated 1.7 million brain injuries suffered in the United States annually — many of them from falls and auto accidents. More than 300,000 cases of TBI have been diagnosed in the military since 2000, along with another 100,000 cases of post-traumatic stress disorder — another condition that Morries and Henderson have attempted to treat with their laser. Both TBI and PTSD are considered major contributors to the high rate of suicide among vets, estimated at more than twenty per day. Finding new approaches to recovery that work has become one of the most urgent quests on the frontiers of neuroscience.
But are the Centennial doctors destined to be trailblazers on that frontier, or are they being consigned to its fringe? At the same time that Morries and Henderson are trying to raise money for further research through benefit dinners, pleas on their website and a GoFundMe campaign, the University of Colorado Anschutz Medical Campus is preparing to launch its own cutting-edge institute dedicated to TBI research and veterans’ mental-health issues, fueled by a $38 million gift from a single foundation.
Henderson suggests that the disparity in funding says more about the power of academia in setting the agenda for medical research than it does about the merits of laser therapy. “Not being university-affiliated is a big part of it,” he sighs. “If someone at CU sneezes, it’s in the Denver Post.”
Henderson believes so strongly in the merits of the laser that he’s willing to head into the valley of debt to get a double-blind, placebo-controlled trial under way. “Right now I’m exploring how I can get a $250,000 loan to start the study,” he says. “If we wait around for the NIH [National Institutes of Health] to fund this, it’s going to be four years. These veterans don’t have four years. We need to do the study now.”

Henderson and Morries use brain scans to help determine where to target the laser during treatment.
Courtesy of The Neuro-Laser Foundation
A belief in the healing power of light is as old as the pyramids. The modern science of light therapy can be traced back to a sickly nineteenth-century researcher named Niels Finsen. A Danish-educated native of the Faroe Islands, Finsen suffered from a rare lipid disorder; sun baths seemed to be one of the few treatments that helped. He began to explore the effect of different wavelengths of light on other conditions, including using ultraviolet light to battle a disfiguring skin infection caused by tuberculosis."When you look at the cost benefit, to have your spouse back - how do you put a price on that?"
tweet this
In 1903, Finsen was awarded the Nobel Prize for his research. It’s not clear that he fully understood the processes by which his results were achieved — the benefits of his assault on the tubercular condition, for example, may have had less to do with ultraviolet light than with oxygen generation — and much of his work was quickly superseded by the development of antibiotics and vaccines.
But Finsen pointed the way, and subsequent technological advances, such as the development of the laser in the 1960s, opened exciting new avenues of research. Today, lasers and other light devices are extremely common in dermatology, from treating acne or skin cancer to tattoo removal. A slew of studies have explored the uses of near-infrared light therapy (NILT) in treating inflammation, strokes, neuropathy and even depression. The results have been decidedly mixed — in part, some researchers say, because of the bewildering array of light sources, wavelengths, intensities and other “illumination parameters” that different groups have chosen to champion in their research.
Larry Morries began using a laser in his South Broadway office seven years ago. A longtime chiropractor in the Denver area — his state chiropractic and electrotherapy licenses date back to 1973 — Morries found that laser sessions, in addition to his standard treatments, seemed to do more to improve lower back pain and joint problems than the standard treatments alone. His interest in the field soon prompted him to seek out Michael Hamblin, a Harvard professor and principal investigator at the Wellman Center for Photomedicine at Massachusetts General Hospital, regarded as one of the world’s top researchers in near-infrared therapies.
Among other projects, Hamblin had been involved in studies suggesting that exposure to NILT could benefit people suffering from depression and anxiety disorders. But it struck Morries that many of the studies dealt with low-powered or “cold” lasers; he believed a higher-wattage laser could have more dramatic and lasting benefits, if it was able to precisely zero in on the area of damage.
Morries broached the idea with Henderson, a psychiatrist who also had some training in radiology — and a strong interest in TBI cases. Henderson was an ardent proponent of a brain-scanning technology known as SPECT (single-photon emission computed tomography), which yields detailed images of the brain, similar to an MRI or PET scan. Morries figured that SPECT images could be extremely useful in targeting problem areas of the brain.
“He knew there was something there, and so did I,” Morries says. “It hit us both in the head that this was a great chance to combine our efforts. He could show me where I needed to aim the laser to have an effect on the neurological cells.”
Henderson says he was slow to embrace the idea. “This guy comes to me, a chiropractor, saying we need to do SPECT scans to show that this laser thing actually helps brain injury,” he recalls. “I thought, ‘What a hunk of malarkey. Nonsense. Gobbledygook.’ Then I read everything Hamblin had done.”
The biochemical mechanisms by which NILT is supposed to improve brain function aren’t entirely understood. The most widely advanced theory is that radiant energy from the light device stimulates mitochondria, which in turn trigger various chemical reactions in the brain — including the production of ATP, a molecule essential to many cellular processes, and increased activity by growth factors and “early response genes” involved in tissue repair. But in reviewing the literature on the subject, Henderson, like Morries, saw some major drawbacks in using low-powered light sources to get this chemical cascade started. Many of the studies involved animal subjects, typically mice. Reducing a lesion in a rodent’s brain with a milliwatt cold laser might not be a big deal, but could such a device transfer energy through something as thick and obdurate as a human skull?
“The science was there,” Henderson says. “The question was whether you could get it in the human head.”
In 2015 Henderson, Morries and Paolo Cassano, a psychiatrist at Massachusetts General, published a study that addressed that question in a novel way. Their team inserted light meters in the heads of freshly slaughtered lambs in order to measure the degree of penetration by light emitted from various near-infrared devices. They also studied light penetration through other tissues, including the human hand. They found that higher-wattage lasers achieved at least three centimeters of penetration through skin and bone, without heating or damaging tissue. Lower-powered devices, such as LED devices used in some NILT studies, failed to penetrate.
Henderson says the penetration study has been accessed online more than 20,000 times since its publication, an indication that others in the research community are paying more attention to what the Neuro-Laser Foundation is doing than they might like to admit. More important, he says, the study demonstrates that their technology is superior to that of many of their competitors in TBI treatment and research.
“These milliwatt LED things — that yahoos here in town and elsewhere say they’re using to treat traumatic brain injury — don’t even get through the skin,” he declares. “LEDs are great if you’re trying to treat the skin. LEDs for acne? Wonderful. But if you’re trying to treat the brain, you’d better get serious.”
“They don’t work, and that’s the bottom line,” Morries adds.
The VA’s office of research and development is currently funding a clinical trial involving the use of an LED device for treating TBI. (A principal investigator in that study didn’t respond to a request for comment.) Henderson says the long process of obtaining federal funding makes it difficult for researchers to change course in the wake of conflicting findings.
“People get highly invested in what they’re researching, to the point where they don’t see the forest anymore,” he says. “Science moves slowly. We stack up more and more data, and people are still clinging to their old approach.”
In other studies that he co-authored, Henderson has shown that SPECT imaging can be used to distinguish PTSD from TBI in civilian and military patients with a high degree of accuracy, despite similar (and, in some cases, co-existing) symptoms. He and Morries have also published two papers documenting that TBI patients treated with their high-powered laser reported a decline in some symptoms, from headaches and sleep disturbance to anxiety and irritability. But both of those papers are based on extremely limited data; one study group consisted of ten patients, while the other was a case report on a single individual.
Even if the number of patients involved was larger, self-reported claims of improved mood or sleep don’t constitute objective proof that the laser sessions are “giving damaged brain cells new life.” In many TBI cases, symptoms tend to improve in time, and no researcher can rule out the possibility that a certain percentage of patients report feeling better because of a placebo effect — not without a controlled study. Morries and Henderson readily concede that until they can afford to conduct such a study, it’s easy for others to discount their work.
“Placebo rates vary in medication trials from 15 to 40 percent,” Henderson notes. “It’s impossible for us to say how much of this is that we’re just really good salesmen. That’s why the double-blind, sham-controlled trial is so important.”"It's impossible for us to say how much of this is that we're just really good salesmen."
tweet this
But that doesn’t mean the anecdotal data provided by the brain-lasered patients isn’t intriguing in its own way. The case report that focuses on just one patient, for example, details how the subject continued to experience symptoms of a moderate TBI a full thirty years after a traffic accident. He had recurrent headaches, swung his right leg outward when walking, had troubles thinking and speaking coherently, and wrote word-clanging, cryptic poetry, riddled with acronyms. (Sample: Two dupes and a coward TDC gather outlier district concert depravities, finding it ODD that what is gone still seeds the mind horizontally. Gravity and grace both lie in trilateral descent to go vertical; inbound products of residents gather by a ghostly tribe of grace instilled.)
After twenty sessions with the laser, the patient’s speech improved notably — and continued to improve in the months after the treatments stopped. So did his gait, his headaches, his sleep, his cognition. “He appeared to have better judgment and was less erratic,” the Morries-Henderson study reports. “His poetry had much less word clanging and a more cohesive line of thought. He moved away from solely writing acronyms to writing sonnets [in] iambic pentameter.”
Another of the doctors’ patients, 36-year-old Kim McCoy, suffered a head injury in an auto accident in Texas three years ago. She spent weeks in a coma; her family was urged to consider donating her organs. Fortunately, her cognitive powers have improved considerably since then, but she still has trouble walking and coping with her emotions. After ten sessions with the laser, she says, “I’ve noticed that I’m happier. I’m thinking better. They’re making me feel more normal. Not as paranoid.”
Carol McCoy, Kim’s mother, reports that her daughter has fewer headaches than when she started the sessions two months ago. And the visit to Colorado had other, unexpected benefits. The doctors who evaluated her after her accident concluded that the brain injury had affected her ability to walk; Morries discovered that she had a previously undiagnosed hip fracture that could be corrected with surgery.
The standard price for twenty laser sessions at the Neuro-Laser Foundation is $4,000. The SPECT scan that’s required before starting treatment costs thousands more. Henderson and Morries offer substantial discounts to military veterans, and some forms of health insurance, such as chiropractic coverage, might defray some of the costs. But many carriers don’t regard laser treatment for TBI as an approved procedure and balk at paying for anything; for instance, while Medicare will pay for a SPECT scan in connection with TBI treatment, Kaiser Permanente considers SPECT an “experimental” technology. Consequently, many patients end up paying for the sessions and scans out of their own pocket, along with the expenses of traveling to Denver and staying here for weeks at a time. The total figure for a full course of sessions can easily exceed $10,000.
Carol McCoy doesn’t know if her daughter will ever be able to “Say Goodbye TBI.” All she knows is that Kim seems “more energetic, more excited about life” since the laser treatments started.
“It’s expensive, but you’ve got to do everything you can to help,” she says. “I don’t know if I could live with myself if I didn’t try.”
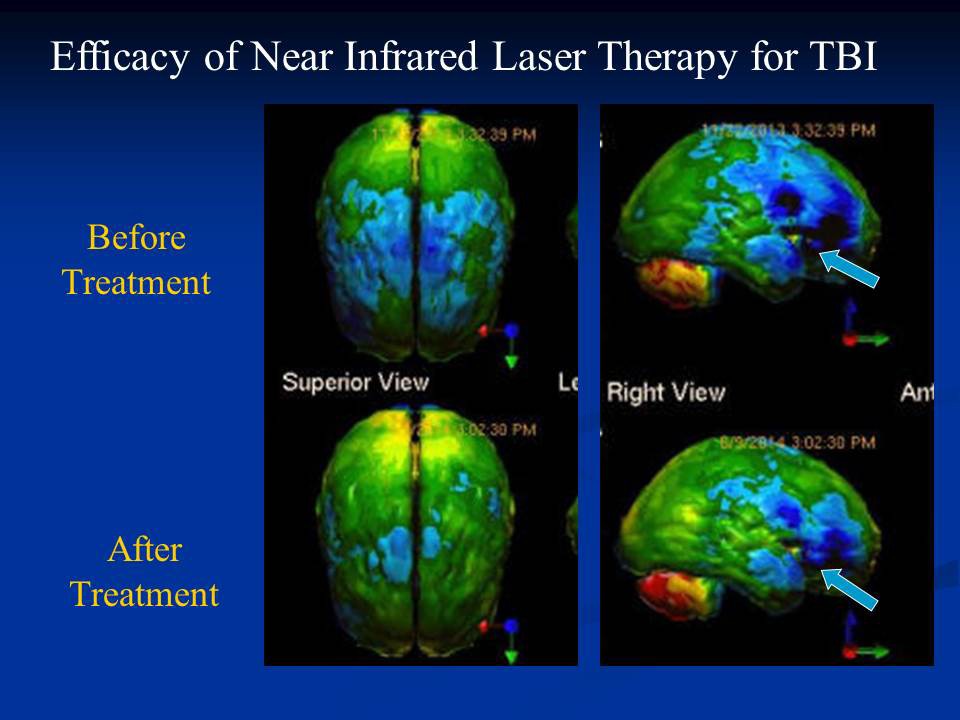
Henderson and Morries reported in one study that brain scans of a TBI patient showed “robust changes in activity” after laser treatments.
Courtesy of The Neuro-Laser Foundation
“All you have to know is that blue is bad and green is better,” Henderson quips, pulling up one series of scans on his desktop computer.
But there is an ongoing debate in neurological circles regarding the use of SPECT imaging as a diagnostic tool, particularly in TBI cases. Critics view the technology, which has been around for decades and primarily portrays the degree of blood flow in the imaged region, as inferior to state-of-the-art processes, and highly limited in application. The colorful 3-D pictures it yields may seem impressive to laymen, but those pictures can’t capture the more subtle aspects of events within the human brain.
A co-author on one of Henderson’s research papers is Daniel Amen, a psychiatrist whose savvy promotion of SPECT as the wonder of the age has made him a celebrity — complete with his own line of best-selling books, television programs and nutritional supplements. Amen claims to have used SPECT imaging to diagnose a range of psychiatric conditions, from depression to autism and attention deficit disorder. As his popular following has grown, so has the debunking from members of the medical establishment, who’ve likened his use of SPECT to palm-reading and phrenology, the Victorian pseudoscience that interpreted the shape of one’s head as an indicator of personality.
Henderson says that he, too, was critical of Amen years ago because of the lack of empirical research to back up his claims. But he believes that Amen is now “doing the science” to support his approach. Henderson has published several papers on the virtues of SPECT and is the president of the International Society of Applied Neuroimaging, a group of a hundred or so members who seem committed to SPECT as a practical tool in the field — and one that’s less expensive than many of the alternatives.
“The neurologists resist it, and they will to their dying day,” Henderson says. “SPECT should be accepted as a diagnostic tool, in my opinion. The data is there. But there’s politics involved.”
Unlike an MRI, a SPECT scan involves the injection of a radioactive isotope into the patient. That troubles Harriet Hall, a retired family physician and former Air Force flight surgeon who’s written skeptically about Amen and SPECT for the Quackwatch website and other online forums. Asked by Westword to review the Henderson-Morries case report on the word-clanging patient, which uses SPECT images to show “robust changes in activity” in the brain following laser treatments, Hall says she wasn’t impressed.
“What matters is the clinical improvement, not the SPECT changes,” Hall says. “I see SPECT as an unnecessary and expensive gimmick, and one that exposes patients to radiation.”
Henderson responds that the amount of radiation involved in a SPECT scan amounts to what a person would be exposed to flying from New York to Los Angeles a couple of times. He points out that a PET scan also involves the use of radioactive tracers, and he insists that SPECT imagery is valuable in determining where to target treatment and in gauging results.
“Blood flow, particularly arterial blood flow, follows function — with very few exceptions,” he says. “There’s the ability to say, ‘Here’s where the injury is, this is where you target.’ And to show the difference [after treatment]. SPECT is a difference engine.”

Neurologist James Kelly, an expert on concussions and TBI, heads a new brain-injury treatment program at the University of Colorado Anschutz Medical Campus.
Eric Stephenson Photography
A former Colorado Springs police officer named Carlos — out of privacy concerns, his family asked that only his first name be published — found out about the hidden hazards of the job back in 2003, when he was in his early thirties. He was in uniform and on his way to work in his own car. At a red light, he glanced in his rearview mirror and saw an altercation developing between the occupants of a van and others in a convertible. He called it in, but before backup could arrive, the van group descended on the convertible with baseball bats.
Carlos got out of his car, drew his weapon and started barking commands for the attackers to get on the ground. Some complied, some didn’t. Somebody said there was a man in the van with a gun. In the tense standoff that followed, the man refused to exit the van and tried to drive away, even though one of the prone suspects was directly in his path. Carlos lowered his weapon, drew a knife and popped a tire. Then, as if on cue, the cavalry arrived.
It was over in seconds, but Carlos kept replaying those seconds in his mind. “I didn’t realize how much it bothered me until a week later,” he recalls. “I could see my hands shaking. I was feeling nervous going on certain calls. I didn’t know anything about PTSD or depression or anything else.”
Eventually he told a lieutenant that he was depressed. The man stared at him blankly and asked for his gun. The department took him off the streets briefly, sent him to a psychiatrist, then okayed his return to patrol. He saw worse things: a young girl run over in the streets. A boy his son’s age who shot himself in the head, so much blood everywhere. A dead baby he was asked to deliver to the hospital morgue. In 2007 he was among the first responders after the New Life Church shootings, which claimed the lives of two teenage girls.
He felt his insides clenching up in crowds or in response to loud noises or sirens. Worse, his memory began to fail him; it was as if all these bad images he didn’t want were crowding out stuff he needed. He couldn’t remember the code for the garage, his kids’ names, or just words he needed every day, elusive words for whatchamacallit. “There were people who thought I was actually drunk,” Carlos says. “I couldn’t get out what I wanted to say.” His wife, Geri, a nurse, told him he was acting like someone experiencing the onset of Alzheimer’s.
Four years ago, he was sitting with other patrol officers in the station house, watching a required training video. The officer in the video got shot, and Carlos went into a full-blown panic attack, crying uncontrollably and feeling like he was going to pass out. “That was pretty much the end of my career,” he says. “I had to fight to get my disability.”
After fifteen years as a cop, he was 42 and unemployed. Over the next two years he grew less verbal, more withdrawn and depressed. There were so many triggers out there, sights and sounds and smells, that he preferred to stay in his house. But even there, he had trouble focusing. He would start to say something, then forget what he wanted to say. The mounting frustration made him angry, sometimes suicidal. Another ex-officer suggested he check out the Neuro-Laser Foundation.
Geri remembers watching in alarm as Henderson conducted an initial evaluation of her husband. Carlos couldn’t count backward from 100; it took him two or three minutes to get to the fourth number, and then he gave up. “He couldn’t converse with someone,” she says.
After several weeks of laser sessions, Carlos “started to feel my personality coming back,” he remembers. He’s now visiting the clinic once a month for additional treatments. He says his memory and verbal abilities have improved. He’s better able to anticipate situations that might trigger panic attacks and avoid them, and he’s in the process of developing a business that recycles discarded wood into furniture.
Geri says the physicians she works with are skeptical of the benefits of the treatments, but she figures it’s cheaper than hospitalization. “When you look at the cost benefit, to have your spouse back — how do you put a price on that?” she asks. “He can cope now, where before he couldn’t. He’s more himself.”
Carlos’s condition didn’t result from any kind of physical injury to the brain. As in the case of a TBI, the jury is still out on how effective laser therapy might be in the treatment of depression and PTSD. Henderson has his theories about why the same treatment he uses on TBI patients is helping Carlos, “but until we actually do the research on PTSD, it’s challenging to speculate,” he says. “That’s a future study.”
Brain chemistry is complex, and doctors like to say that every case is different and requires an individualized response. Because symptoms can vary widely, even the process of diagnosis can be difficult. Last year the VA admitted that it may well have misdiagnosed 24,000 veterans whose exams for possible brain injuries were performed by physicians not qualified to diagnose TBI.
“We don’t have an approved, accepted biological test that says you’ve had a concussion,” notes James Kelly, a neurologist who teaches at the University of Colorado Anschutz Medical Campus. “We don’t have that on traumatic brain injury, either — especially at the mild end of the spectrum.”
Kelly has long been recognized as one of the country’s top experts on treating concussions, dating back decades to pioneering research that helped establish protocols for monitoring athletes and guidelines for concussion management. While on leave from CU, he headed the National Intrepid Center of Excellence, a recently established program at Walter Reed dedicated to helping active-duty veterans of the Iraq and Afghanistan conflicts who had TBIs and psychological issues. His work there attracted the attention of Bernard Marcus, one of the founders of the Home Depot and a strong supporter of vet recovery programs. The result was a $38 million gift from the Marcus Foundation to establish the Marcus Institute for Brain Health at the CU Anschutz campus in Aurora, with Kelly as the institute’s executive director.
The facility, which is expected to open later this summer, will offer patients and their providers an impressive range of options, from sophisticated diagnostic equipment to alternative therapies, including acupuncture and yoga. Nearly 20 percent of the Marcus donation will be used to purchase cutting-edge neuroimaging technology, such as susceptibility weighted imaging machines, an advanced form of MRI that tracks iron deposition or “staining” in the brain from broken blood vessels, allowing physicians to better pinpoint areas of neuronal injury. None of the new machines use SPECT, which Kelly describes as “a good example of something that’s tough to pin down as to its usefulness.”
Kelly won’t comment on the merits of laser therapy, saying he isn’t sufficiently familiar with the research to venture an opinion. He says his own experience has shown him that there’s no magic bullet for traumatic brain injuries and PTSD, but many patients can recover by incremental degrees with time and judiciously developed forms of intervention, from techniques to improve sleep to ways of aiding memory and concentration.
Combining conventional treatment with alternative therapies “allows you to personalize health care around the individual’s constellation of problems,” Kelly says. “Everything I had at Walter Reed is on this campus. Every individual gets a detailed evaluation, and we’re not guessing. We can target their care.”
Henderson recalls attending a presentation at a psychiatric conference on the program Kelly developed at Walter Reed. What struck him about the exit interviews conducted with patients, he says, is that “what they liked most was the dog therapy and the acupuncture.” That raises a basic question, he suggests, about whether mainstream medical interventions for TBI are truly of more benefit than so-called feel-good measures.
Of course, the same could be said of the laser sessions offered by Henderson and Morries. Until a controlled study is conducted, who’s to say if the laser works, or if the claimed improvements are the result of diet, massage or the healing hands of time? That’s one reason that Henderson was at the Society of Nuclear Medicine and Molecular Imaging annual meeting last month, trying to drum up support for the planned double-blind clinical trial.
The meeting happened to be in Denver this year, but Henderson would have gone even if it had involved a flight to Tampa or Poughkeepsie. “I attend them every year,” he says, “and I know all the big players.”